Cervical Spondylosis & Treatment
A Pain In The Neck!
Neck pain may be attributed to a variety of factors, including muscle strain, ligament sprains, arthritis of neck joints or degenerative in nature, commonly known as cervical spondylosis. Approximately 10 percent of adults have Cervical spondylosis at any one time. Fortunately, most patients, regardless of the cause of pain, get better with conservative therapy.
Structures in the neck
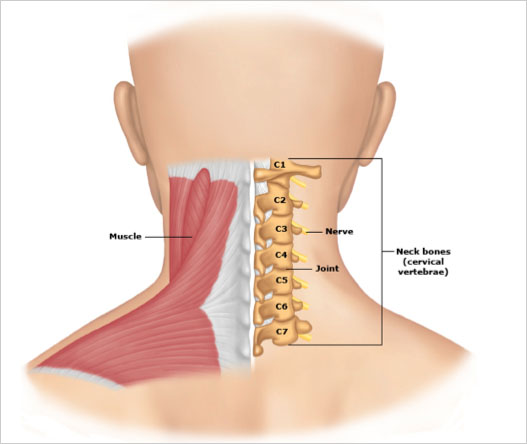
In order to better understand your cervical spondylosis, it is useful to identify some basic structures that it comprise of. The neck, or cervical spine, is formed by seven square-shaped bones (cervical vertebrae), which are stacked one on top of another. The vertebrae are named for their position in the cervical spine, beginning at the top with C1 down to C7. Together with the supporting ligaments and the overlying long neck muscles, the cervical vertebrae form a spinal canal that surrounds and protects the spinal cord (Figure 1).
In between the neck bones are discs, which function as shock absorbers, cushioning one bone from another. Directly over the bones and the discs is a layer of strong ligaments. These thick tissues are attached directly to the bones and function to limit the movement of one vertebra against the other. Car accidents and injuries to the head or body can cause injury to these ligaments and the joints that it supports.
Overlying the small muscles that support the vertebrae, the major muscles of the neck form the next protective layer. These muscles are responsible for holding the head up, maintaining normal posture, and supporting the neck. Overuse and irritation of these larger muscles is often called neck strain. Muscular strain is not cervical spondylosis.
Cervical spondylosis — Cervical spondylosis is a common term used by doctors to refer to degenerative changes (wear and tear) of the cervical spine. Wear-and-tear causes gradual narrowing of the disc space, a loss of the normal square-shaped bone, and growth of the edges of the bone (bone spurs). These spurs can increase pressure on the surrounding tissues. Some degree of wear and tear is normal with aging, although severe degenerative changes are not normal. In other words, having Cervical spondylosis as a result of degenerative changes does not mean it cannot be treated.
- Cervical discogenic pain — Cervical discogenic pain may be one of the most common cause of Cervical spondylosis. It is caused by changes in the structure of one or more of the cervical intervertebral discs. Common symptoms of discogenic pain include pain in the neck when turning or tilting the head. Pain may be worsened when the neck is held in one position for prolonged periods, such as occurs with driving, reading, or working at a computer. Discogenic pain can also refer pain or uncomfortable sensations into the arm or shoulder.
- Cervical facet syndrome — The facet joint, which is located on the left and right side of the vertebrae, is the most commonly affected area in whiplash-related Cervical spondylosis and headaches. Another potential cause of cervical facet syndrome includes a job that requires a person to repeatedly extend the neck (tilt the head backwards). Symptoms of cervical facet syndrome include pain in the middle or side of the neck; some people also notice pain in the shoulders, around the shoulder blades, at the base of the head, or in one arm.
- Cervical stenosis — Cervical stenosis occurs when there are degenerative changes that narrow the central (middle) spinal canal. This narrowing can injure the cervical spinal cord or cause it to function improperly. Weakness, difficulty walking or coordinating movement, inability to empty or control the bowels or bladder, and sexual dysfunction (eg, erectile dysfunction) may occur as a result of irritation or compression of the spinal cord.
- Cervical radiculopathy — Cervical radiculopathy occurs when a nerve root is irritated by a protruding disc, arthritis of the spine, or a mass that compresses a nerve. Signs of radiculopathy can include pain, weakness, or changes in sensation (eg, numbness, pins and needles) in the arms.
How Is Cervical Spondylosis Diagnosed?
The evaluation of Cervical spondylosis usually begins by observing the person’s ability to turn the head to the left and right, forward and backward, and side to side. Your specialist doctor will observe the posture and movement of the neck and shoulders. He will feel the muscles in the neck, head, upper back, and shoulders to detect areas of pain, weakness, or tension. If weakness or sensory complaints are present, strength and sensation in the extremities will also be examined.
In some more complex cases, further testing, such as an x-ray, magnetic resonance imaging (MRI) or electrodiagnostic testing (EMG or electromyography) will be recommended. Even though most cases of Cervical spondylosis can be treated conservatively, it is mandatory to see your specialist for anyone with a head or neck injury, inability to control the bowels or bladder, severe pain, numbness or changes in sensation in the arms or legs, or if pain does not begin to improve after one week with treatment at home.
What Is The Prognosis For Cervical Spondylosis?
The outlook for Cervical spondylosis depends on the precise cause. Most forms of Cervical spondylosis can resolve with conservative measures including rest, avoiding re-injury, and gradual rehabilitation.
Can You Prevent Cervical Spondylosis?
Cervical spondylosis refers to degenerative changes to the structures of the cervical spine that takes place over time. Proper neck posture and good ergonomics may slow down its onset but there is no real way to prevent or avoid it. However, there are some neck stretching and strengthening exercises that will benefit almost everyone.
Stretching exercises — Apart from maintaining flexibility, stretching exercises can also help to decrease pain from muscle injury. Exercises can be performed in the morning to relieve stiffness and again at night before going to bed. Sharp or electric like pain in the shoulder or arm is not normal and should be reported to your specialist doctor.
The most useful stretching exercises for the neck include the following:
- Neck bending — Tilt the head forward and try to touch your chin to your neck. Hold for a few seconds, breathe in gradually, and exhale slowly with each exercise. Exhaling with the movement helps relax the muscles. Repeat 10 to 15 times. Relax the neck and back muscles with each neck bend.
- Shoulder rolls — In the sitting or standing position, hold the arms at the side with the elbows bent. Try to pinch the shoulder blades together. Roll the shoulders backwards 10 to 15 times, moving in a rhythmic, rowing motion. Rest. Roll the shoulders forwards 10 to 15 times.
- Neck rotation — Slowly look to the right. Hold for a few seconds. Look to the center. Rest for a few seconds between movements. Repeat 10 to 15 times. Perform on the left side.
- Neck tilting — Look straight forward, then tilt the top of the head to the right, trying to touch your right ear to the right shoulder (without moving the shoulder). Hold in place for a few seconds. Return the head to the center. Repeat 10 to 15 times. Repeat on the left side.
Vertical shoulder stretches — In the sitting or standing position, use the right hand to hold the left wrist and pull the arm (and shoulder) up and over the head, towards the right. Hold for five seconds. Keep the left shoulder and back muscles relaxed. Rest and repeat 10 to 15 times. Repeat using left hand to hold right wrist.
Upper back stretches — In the standing position, lean forward from the hips and rest both hands on a low counter with the elbows straight. Exhale, relax the neck and shoulders, and allow the head to fall forward as you round the upper back. This requires the shoulder blades to spread apart and mimics the motion of a cat stretching its back. Exhaling with the motion helps to relax the muscles. Return to the standing position with hands on a counter. Repeat slowly 10 times.
Basic neck strengthening — In the same forward positioning as the upper back stretches, after allowing the head to fall forward, raise the head by looking forwards keeping the neck in a straight line as the upper back and hold for 10 seconds. This trains the neck muscles that keep the neck upright. Repeat slowly 10 to 15 times.
Prevention and Posture — Activities and body positions that prevent or reduce Cervical spondylosis include those that emphasize a neutral neck position and minimize tension across the supporting muscles and ligaments of the neck. Extremes of range of motion, activities, and body positions that cause constant tension should be minimized or avoided:
- Avoid sitting in the same position for prolonged periods of time. Take periodic five minute breaks from the desk, work station, etc. Avoid looking up or down at a computer monitor; adjust it to eye level.
- Avoid placing pressure over the upper back with backpacks, over-the-shoulder purses, or children riding on your shoulders.
- Do not perform overhead work for prolonged periods at a time.
- Maintain good posture by holding your head up and keeping your shoulders back and down.
- Use the car or chair arm rests to keep the arms supported.
- Sleep with your neck in a neutral position by sleeping with enough pillows to keep your neck straight in line with your body. Avoid sleeping on the stomach with the head turned.
- Carry heavy objects close to your body rather than with outstretched arms.
Cervical Spondylosis Treatments
What most patients do not realise is that most cases of Cervical spondylosis can be treated conservatively with over-the-counter pain medications, ice, heat and massage, and strengthening and/or stretching exercises at home.
a. Ice — For some people, ice can reduce the severity of Cervical spondylosis. It can be applied directly to the sore area of the neck. Ice can be frozen in a paper cup, and then the upper edge of the cup can be torn away. The ice should be moved continuously in strokes on the neck muscles for five to seven minutes.
- To control sudden onset muscle tightness, place a bag of ice, bag of frozen peas, or a frozen towel wrapped in a dry towel, on the painful area. The ice should be left in place for 15 to 20 minutes to deeply penetrate the tissues; this can be repeated every two to four hours until symptoms improve.
b. Heat — Heat can help to reduce pain in the neck muscles. Moist heat can be applied for 10 to 15 minutes in a shower, hot bath, or with a moist towel warmed in a microwave. However, acute injuries should utilize ice as the initial treatment. Heat may be used initially for patients who have cold intolerance to ice.
c. Massage — Massage can be helpful for relieving muscle spasm and can be performed after heating or icing the neck. Massage can be done with the hands by applying pressure to both sides of the neck and the upper back muscles, or with an electric hand-held vibrator. The neck muscles should be relaxed during massage by supporting the head or lying down.
Many patients may have also attempted acupuncture, biofeedback, cervical collars, cervical traction and other forms of physical therapy. In particular, some studies have found that treatments that include quick “thrusting” of the neck are associated with serious injury. Aggressive manipulation or adjustments to the cervical spine should be discouraged in elderly patients and those with cervical stenosis. Cervical traction involves the use of weights to realign or pull the spinal column into alignment. Clinical studies have shown that there is no benefit of traction in the treatment of Cervical spondylosis.
Is Surgery The Next Step?
Most practitioners will agree that surgery may not be useful for treating most types of Cervical spondylosis. However, surgery does have a role in relieving symptoms related to a pinched nerve caused by a moderately large herniated disc after a trial of conservative therapy (eg, stretching exercises, physical therapy). Most patients however, will only consider surgery as their last option and as a result, they end up enduring a significant amount of pain in the process.
The good news is that today, modern medicine has a much greater understanding of Cervical spondylosis than previously. As there are many varied causes of Cervical spondylosis, there are also as many options of non-surgical interventions that act as the “missing link” between conservative care and surgical options. As a matter of fact, there are many more options for resolving pain, even for people who think — or have been told — that “nothing else can be done.”
Minimally invasive procedures that target these sources include trigger point injections, diagnostic nerve root blocks, facet joint blocks or radio-frequency ablation, and discography. The choice of procedures will ultimately depend on what is diagnosed as the main cause of Cervical spondylosis in the individual patient.
Dr G himself is a general practitioner but attributed his Cervical spondylosis to degenerative changes in his cervical spine. As a result he suffered from Cervical spondylosis for close to 4 years before deciding to come for treatment. One of the reasons that prompted him to do so was that he started developing gastritis as a result of the painkillers he had been taking. Dr G underwent percutaneous radio-frequency facet joint treatment, performed under X-ray guidance. He had since then stopped taking his pain medications and had also resumed playing golf again.